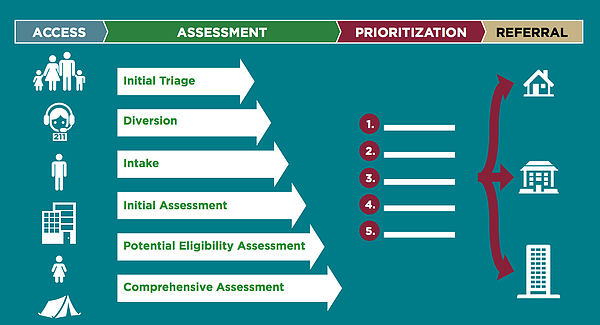
The Coordinated Entry System (CES) is a process which the most vulnerable homeless residents are matched with available and appropriate housing resources. The primary goals for coordinated entry processes are that assistance be allocated as effectively as possible and that it be easily accessible.
Qualities of Effective Coordinated Entry
An effective coordinated entry process has the following qualities:
- Prioritization. HUD has determined that an effective coordinated entry process ensures that people with the greatest needs receive priority for any type of housing and homeless assistance available in the CoC, including PSH, Rapid Rehousing (RRH), and other interventions.
- Low Barrier. The coordinated entry process does not screen people out for assistance because of perceived barriers to housing or services, including, but not limited to, lack of employment or income, drug or alcohol use, or having a criminal record. In addition, housing and homelessness programs lower their screening barriers in partnership with the coordinated entry process.
- Person-Centered. The coordinated entry process incorporates participant choice, which may be facilitated by questions in the assessment tool or through other methods. Choice can include location and type of housing, level of services, and other options about which households can participate in decisions.
- Fair and Equal Access. All people in the CoC’s geographic area have fair and equal access to the coordinated entry process, regardless of where or how they present for services. Fair and equal access means that people can easily access the coordinated entry process, whether in person, by phone, or some other method, and that the process for accessing help is well known. Marketing strategies may include direct outreach to people on the street and other service sites, informational flyers left at service sites and public locations, announcements during CoC or other coalition meetings, and educating mainstream service providers. If the entry point includes one or more physical locations, they are accessible to people with disabilities, and easily accessible by public transportation, or there is another method, e.g., toll-free or 211 phone number, by which people can easily access them. The coordinated entry process is able to serve people who speak languages commonly spoken in the community.
- Emergency services. The coordinated entry process does not delay access to emergency services such as shelter. The process includes a manner for people to access emergency services at all hours independent of the operating hours of the coordinated entry intake and assessment processes. For example, people who need emergency shelter at night are able to access shelter, to the extent that shelter is available, and then receive an assessment in the days that follow, even if the shelter is the access point to the coordinated entry process.
- Standardized Access and Assessment. All coordinated entry locations and methods (phone, in-person, online, etc.) offer the same assessment approach and referrals using uniform decision making processes. A person presenting at a particular coordinated entry location is not steered towards any particular program or provider simply because they presented at that location.
- Inclusive. A coordinated entry process includes all sub-populations, including people experiencing chronic homelessness, Veterans, families, youth, and survivors of domestic violence. However, CoCs may have different processes for accessing coordinated entry, including different access points and assessment tools for the following different populations: (1) adults without children, (2) adults accompanied by children, (3) unaccompanied youth, or (4) households fleeing domestic violence. These are the only groups for which different access points are used. For example, there is not a separate coordinated entry process for people with mental illness or addictions, although the systems addressing those disabilities may serve as referral sources into the process. The CoC continuously evaluates and improves the process ensuring that all subpopulations are well served.
- Referral to projects. The coordinated entry process makes referrals to all projects receiving Emergency Solutions Grants (ESG) and CoC Program funds, including emergency shelter, RRH, PSH, and transitional housing (TH), as well as other housing and homelessness projects. Projects in the community that are dedicated to serving people experiencing homelessness fill all vacancies through referrals, while other housing and services projects determine the extent to which they rely on referrals from the coordinated entry process.
- Referral protocols. Programs that participate in the CoC’s coordinated entry process accept all eligible referrals unless the CoC has a documented protocol for rejecting referrals that ensures that such rejections are justified and rare and that participants are able to identify and access another suitable project.
- Outreach. The coordinated entry process is linked to street outreach efforts so that people sleeping on the streets are prioritized for assistance in the same manner as any other person assessed through the coordinated entry process.
- Ongoing planning and stakeholder consultation. The CoC engages in ongoing planning with all stakeholders participating in the coordinated entry process. This planning includes evaluating and updating the coordinated entry process at least annually. Feedback from individuals and families experiencing homelessness or recently connected to housing through the coordinated entry process is regularly gathered through surveys, focus groups, and other means and is used to improve the process.
- Informing local planning. Information gathered through the coordinated entry process is used to guide homeless assistance planning and system change efforts in the community.
- Leverage local attributes and capacity. The physical and political geography, including the capacity of partners in a community, and the opportunities unique to the community’s context, inform local coordinated entry implementation.
- Safety planning. The coordinated entry process has protocols in place to ensure the safety of the individuals seeking assistance. These protocols ensure that people fleeing domestic violence have safe and confidential access to the coordinated entry process and domestic violence services, and that any data collection adheres to the Violence Against Women Act (VAWA).
- Using HMIS and other systems for coordinated entry. The CoC may use HMIS to collect and manage data associated with assessments and referrals or they may use another data system or process, particularly in instances where there is an existing system in place into which the coordinated entry process can be easily incorporated. For example, a coordinated entry process that serves households with children may use a system from a state or local department of family services to collect and analyze coordinated entry data. Communities may use CoC Program or ESG program funding for HMIS to pay for costs associated with coordinated entry to the extent that coordinated entry is integrated into the CoCs HMIS. A forthcoming paper on Coordinated Entry and HMIS will provide more information.
- Full coverage. A coordinated entry process covers the CoC’s entire geographic area. In CoCs covering large geographic areas (including statewide, Balance of State, or large regional CoCs) the CoC might use several separate coordinated entry processes that each cover a portion of the CoC but in total cover the entire CoC. This might be helpful in CoCs where it is impractical for a person who is assessed in one part of the CoC to access assistance in other parts of the CoC.